Ranexa is indicated as add-on therapy for stable angina in adults inadequately controlled by or intolerant to first-line therapies (beta-blockers and/or calcium antagonists).1

Neutral hemodynamic profile:No significant changes in blood pressure or heart rate.1
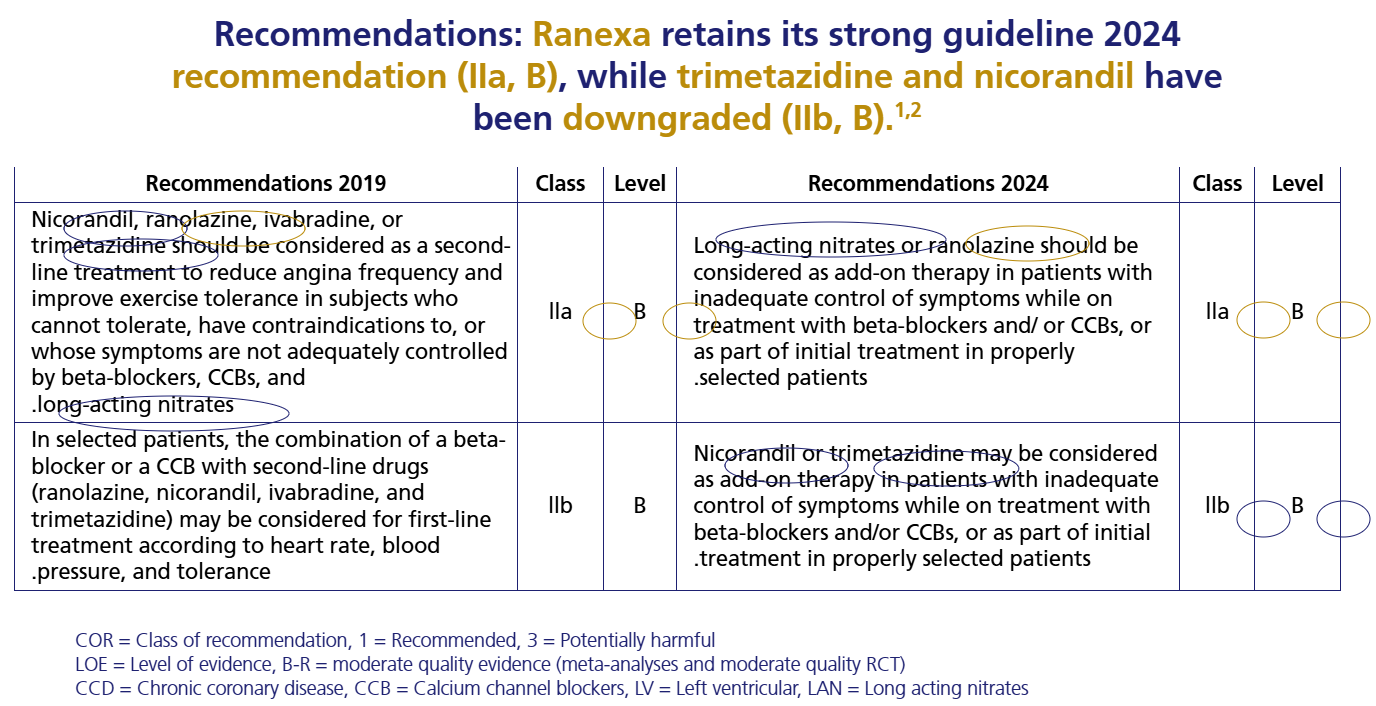
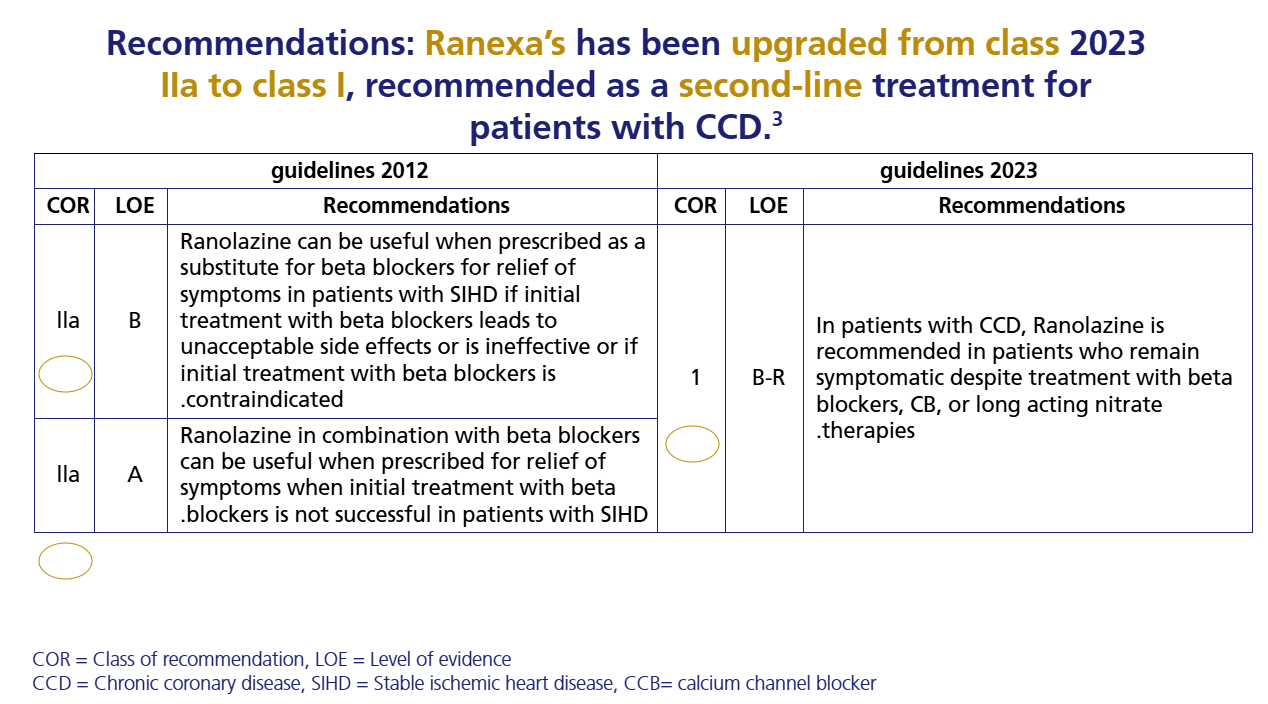
Guideline Recommendation

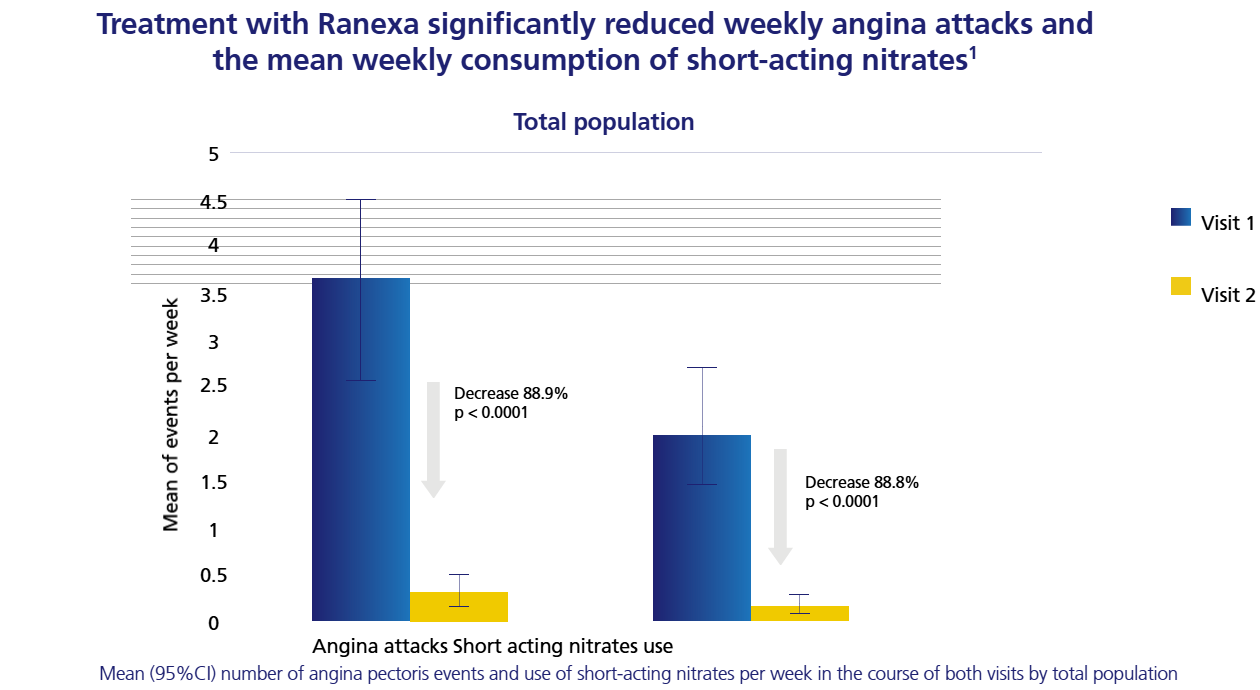
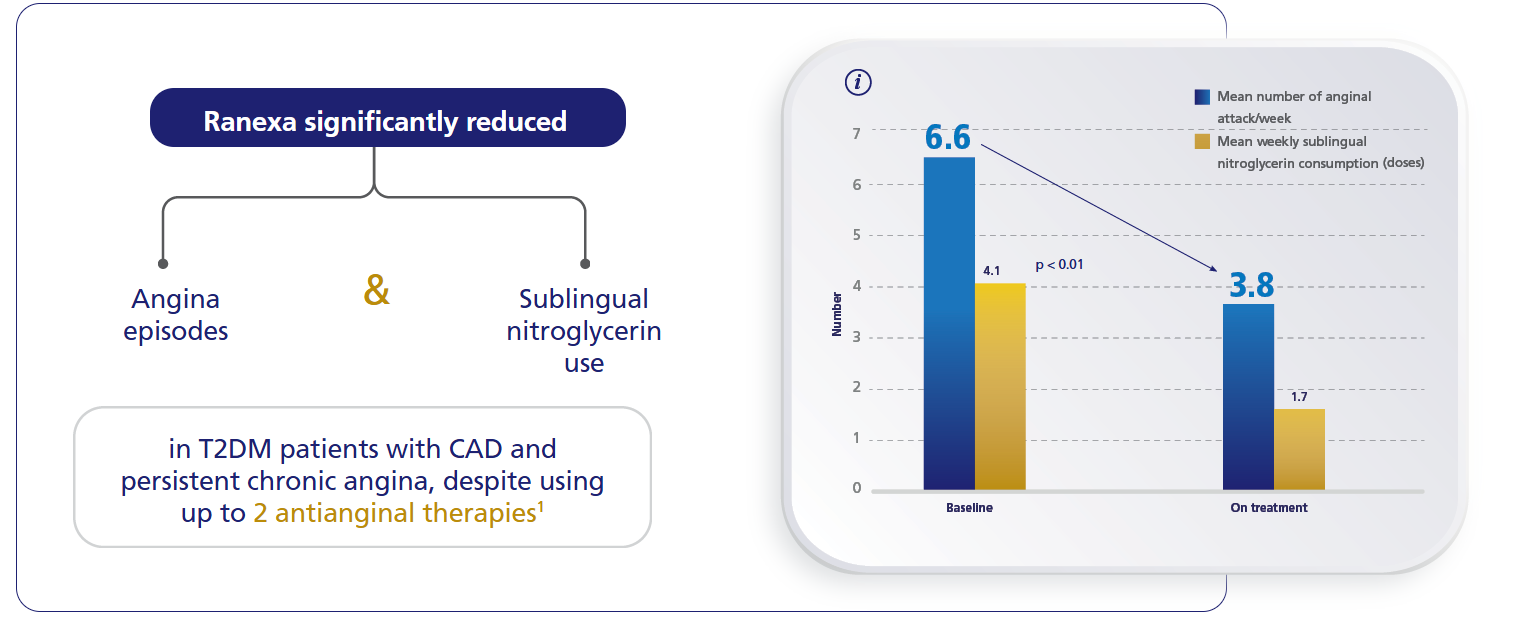
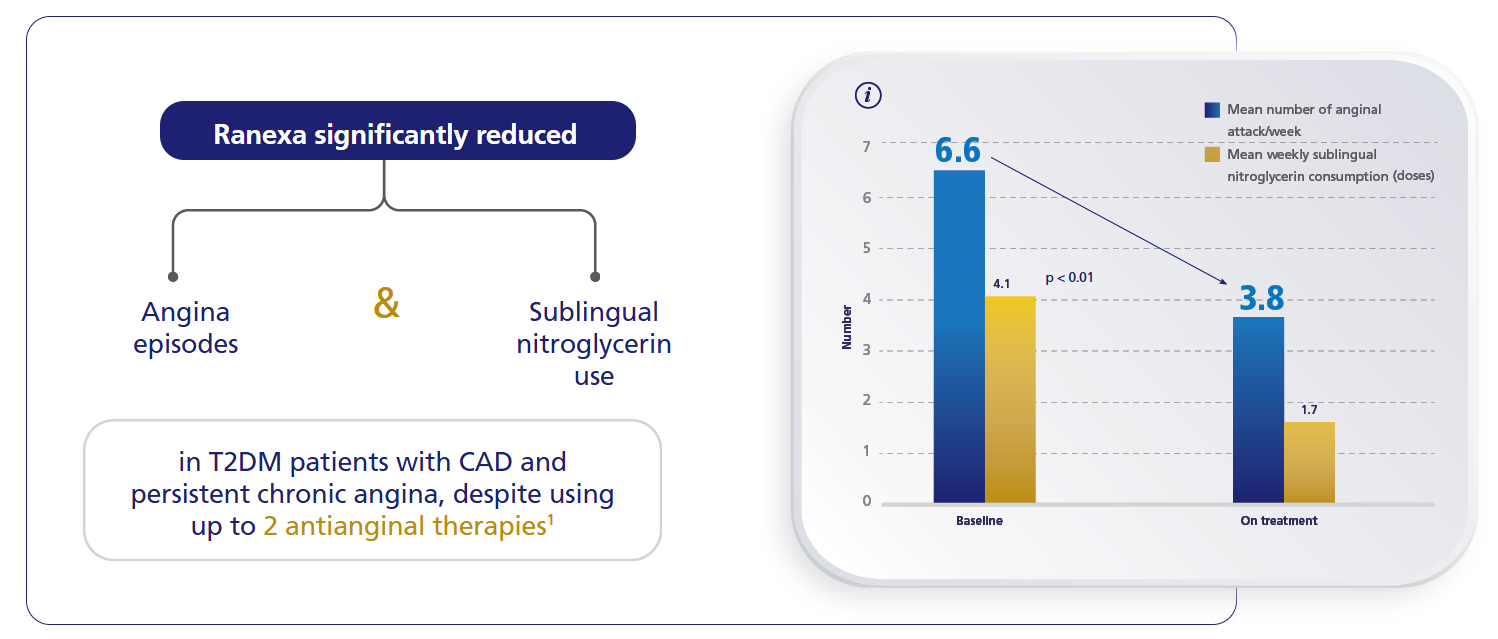
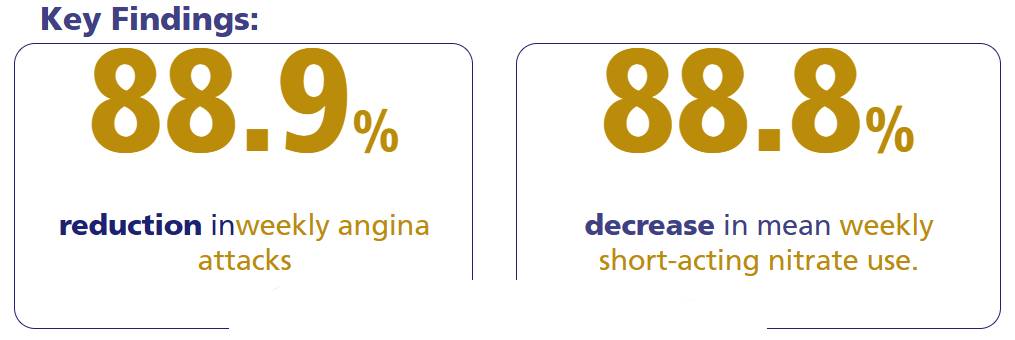
Reduced anginal episodes,
lower nitroglycerin use.6

Strong recommendation retained.7
Neutral hemodynamic profile:No significant changes in blood pressure or heart rate.1
Guideline Recommendation
Reduced anginal episodes,
lower nitroglycerin use.6
Strong recommendation retained.7
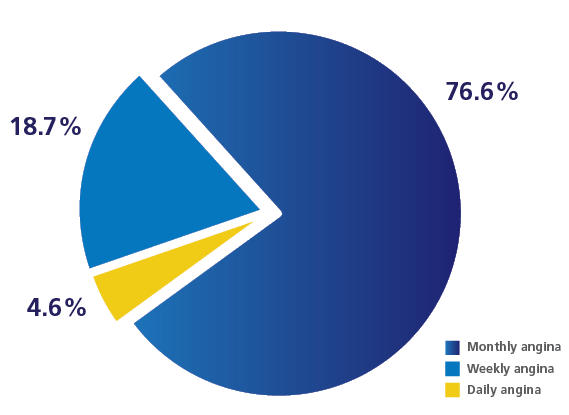
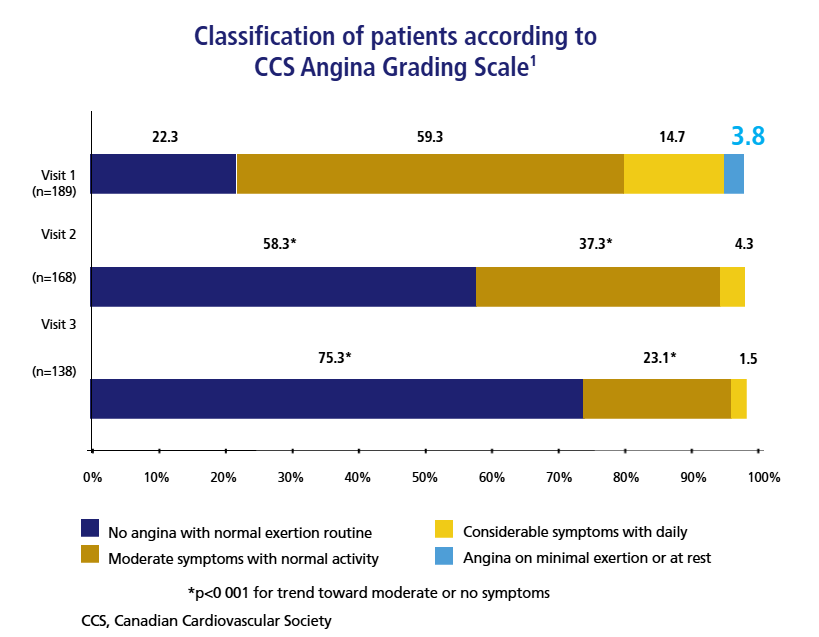
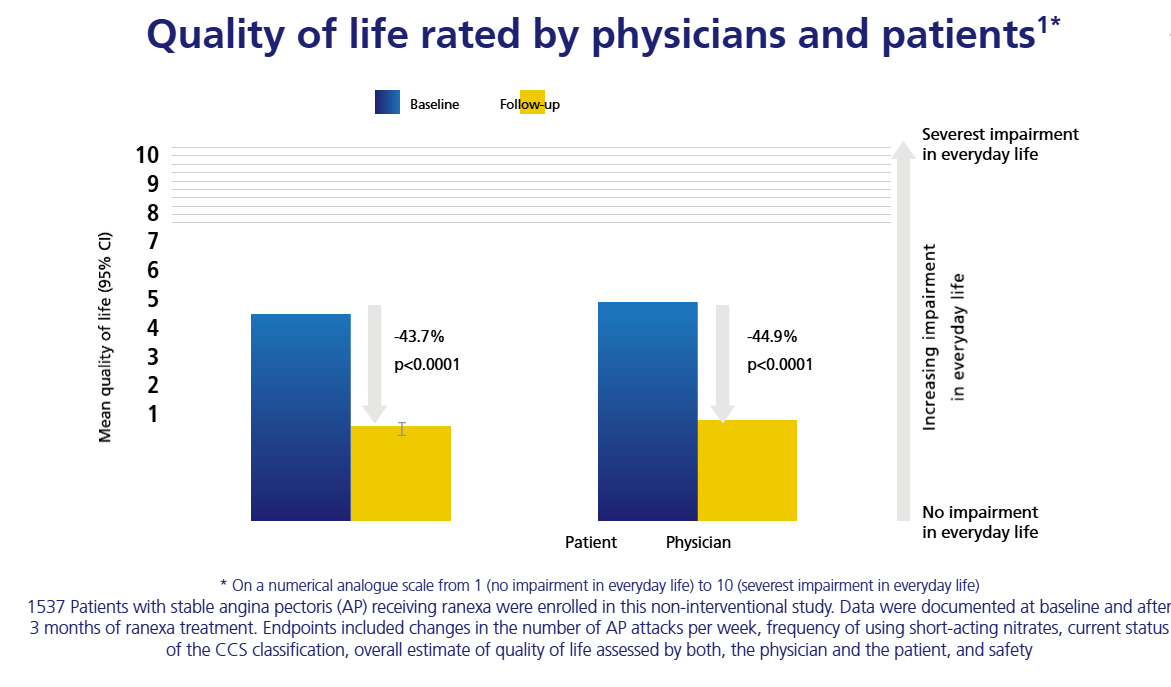
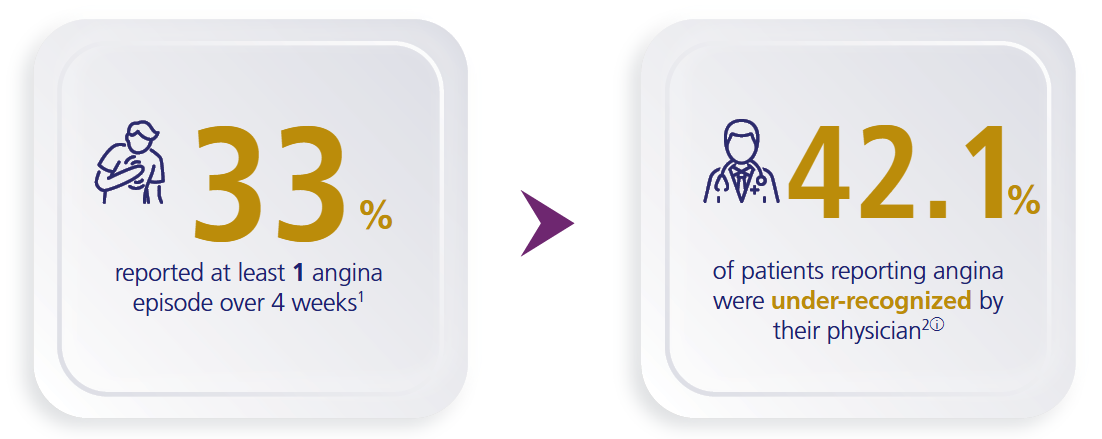
Under-recognition of angina by physicians could affect patients’ quality of life1
APPEAR Study: Among 1257 patients with coronary artery disease

Learn more about:
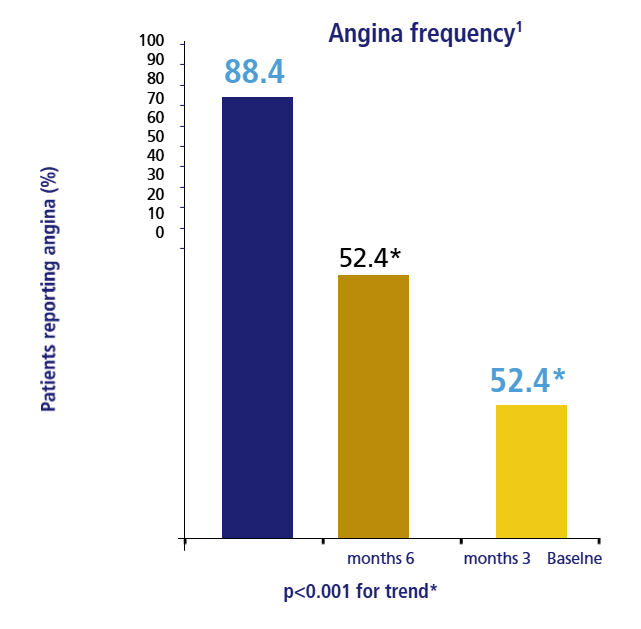
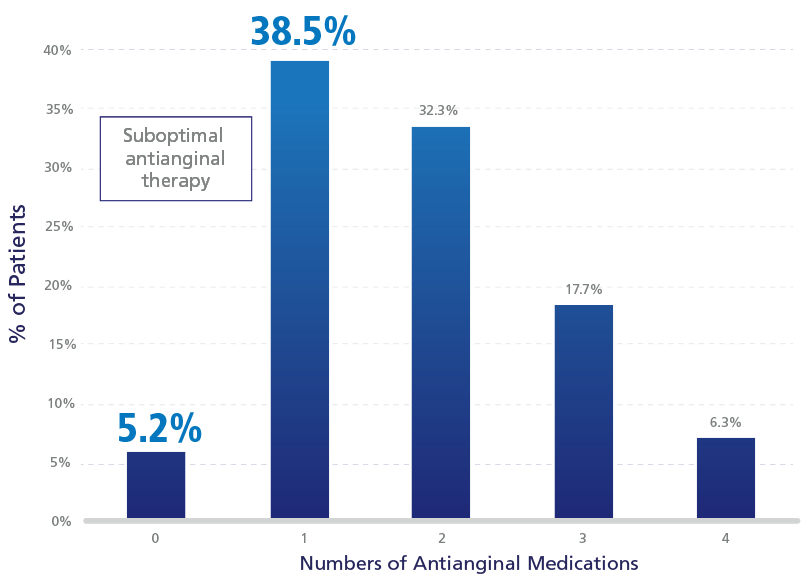
Frequency Distribution of Patient-Reported Angina
APPEAR study: 44% of patients with daily/weekly angina were on suboptimal antianginal therapy.1

For more details
:Key CCS Management Guidelines 2024 Takeaways

Recurrence of Angina After PCI1-6
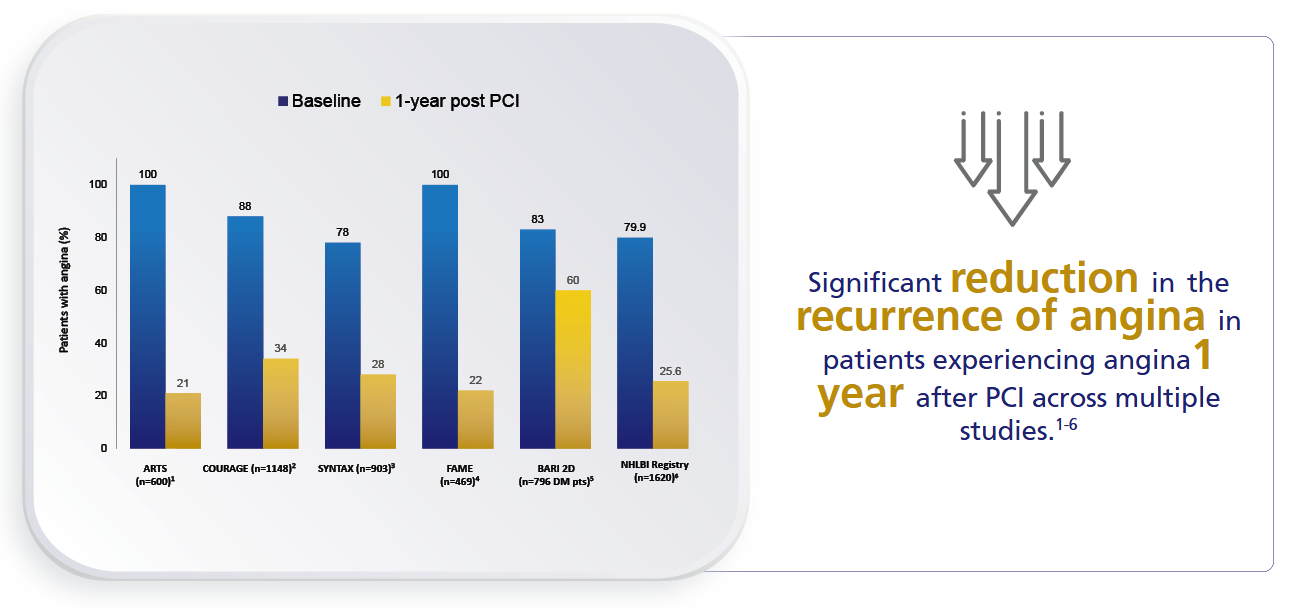

Learn more about: The potential reasons for
persistent angina
Ranexa Patient Profiles
Ranexa: Redefine Life for Your Stable Angina Patients
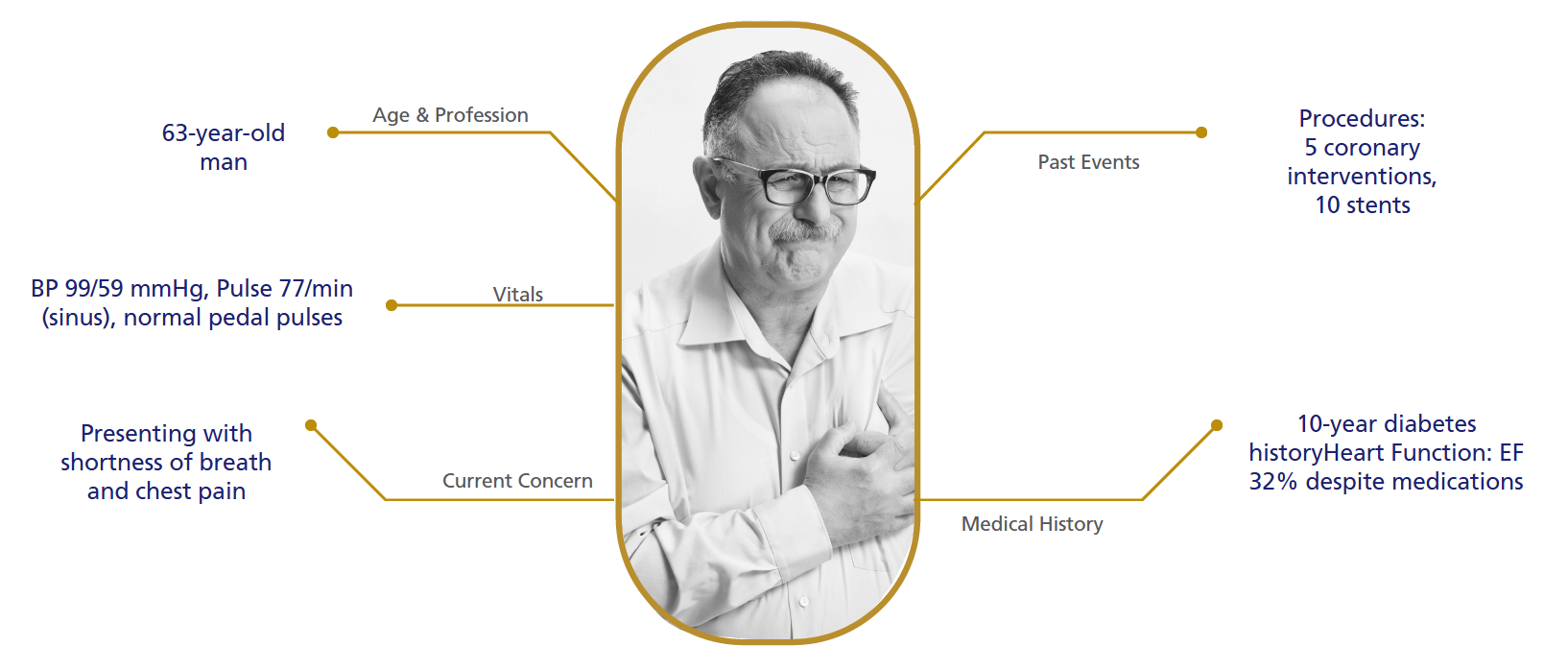
Diabetic Patient with CSA - History
TERISA study1
For more details
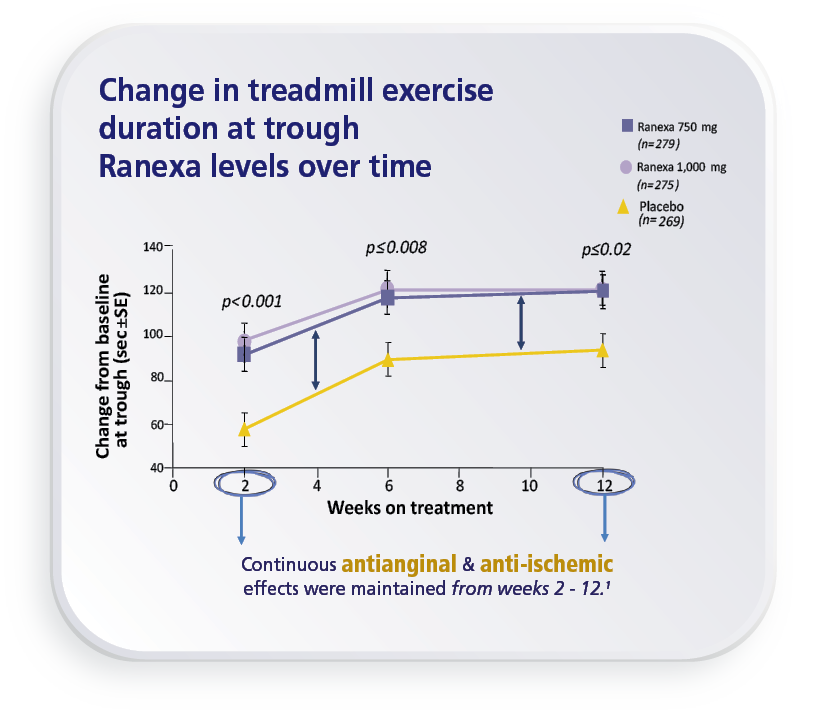
CARISA Study1
Ranexa significantly increased
treadmill exercise duration by 46.3 Sec at peak drug levels.1 (p=0.006)
For more details
CARISA Study1
Ranexa significantly increased
treadmill exercise duration by 46.3 Sec at peak drug levels.1 (p=0.006)
For more details
Diabetic Patient with CSA - History
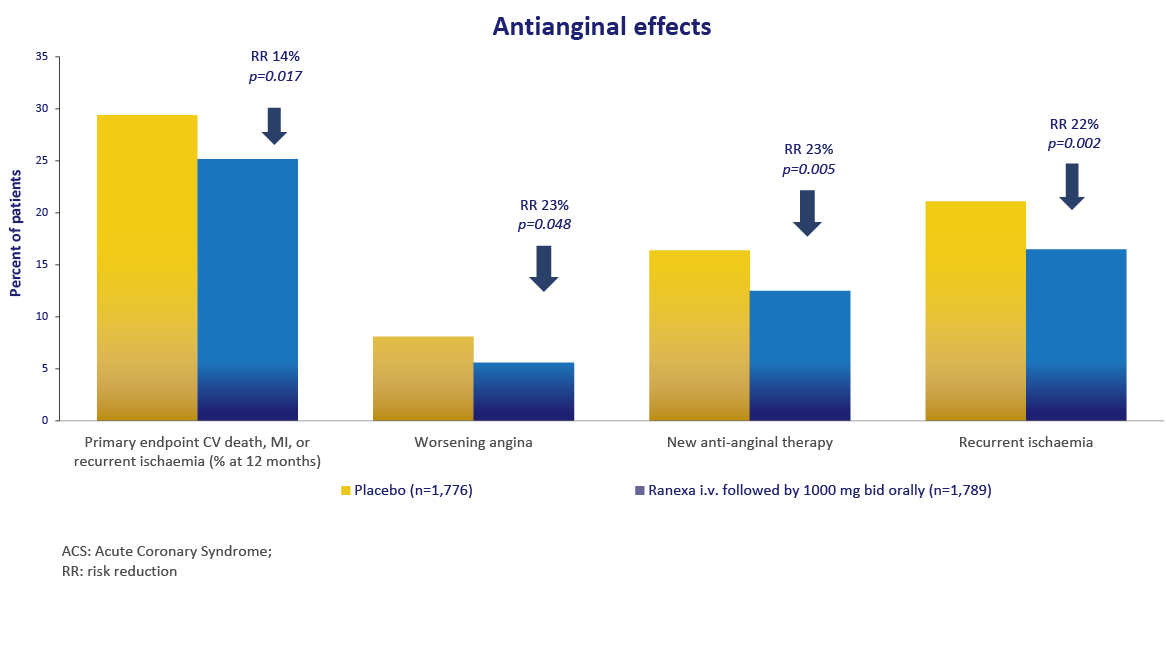
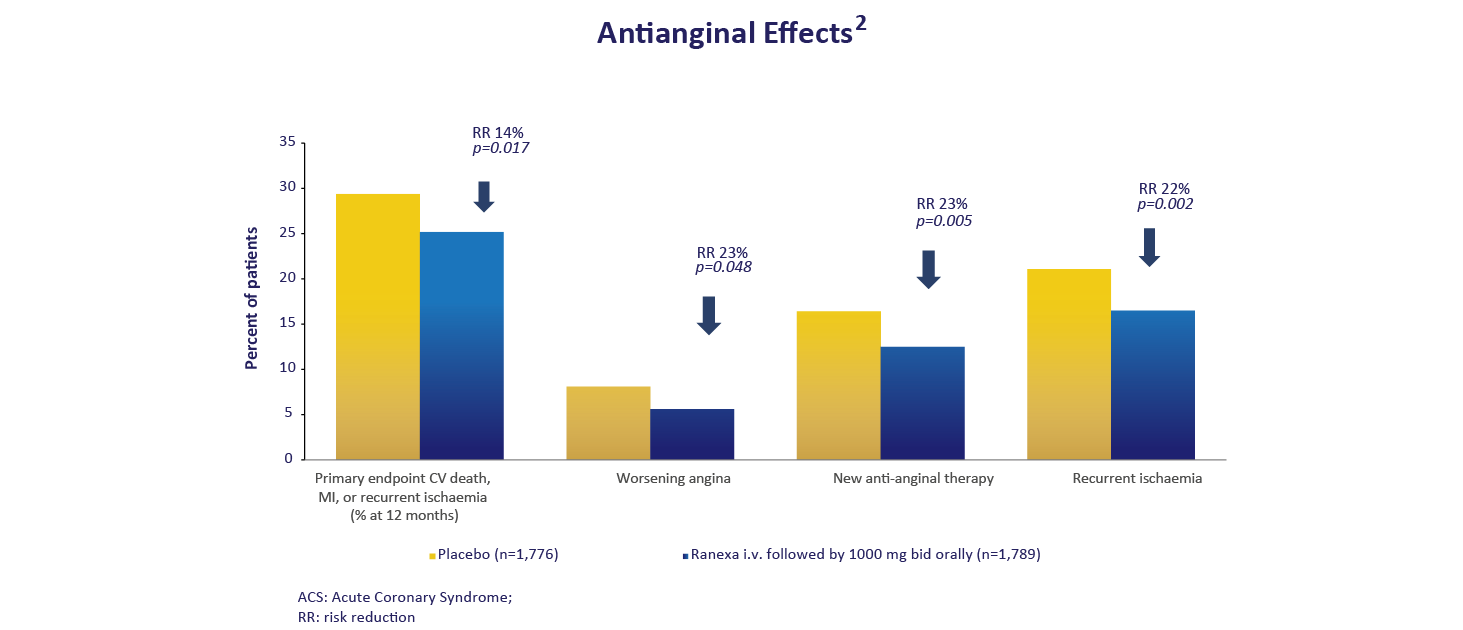
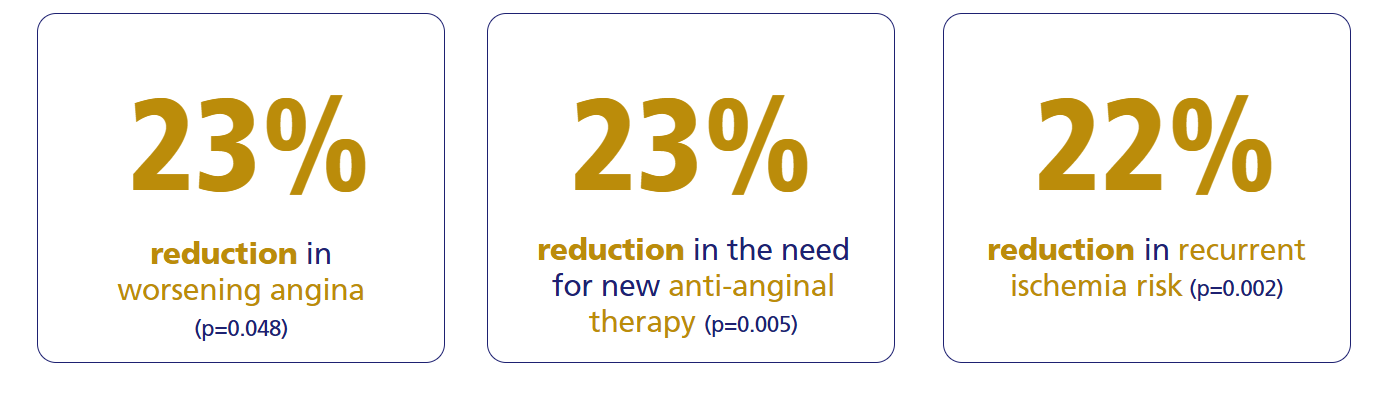
MERLIN-TIMI 36 Study: Ranexa’s Efficacy in Acute
Coronary Syndrome & Chronic Angina1,2
Ranexa significantly reduces cardiovascular endpoints and angina-related events compared to placebo.
For more details
MERLIN-TIMI 36 Study1

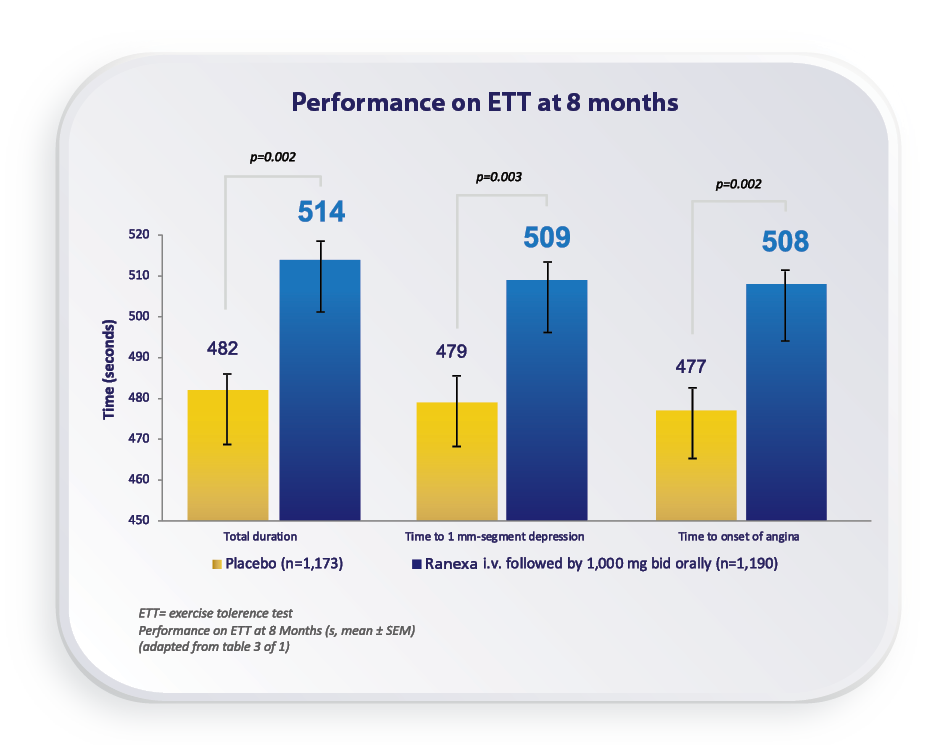
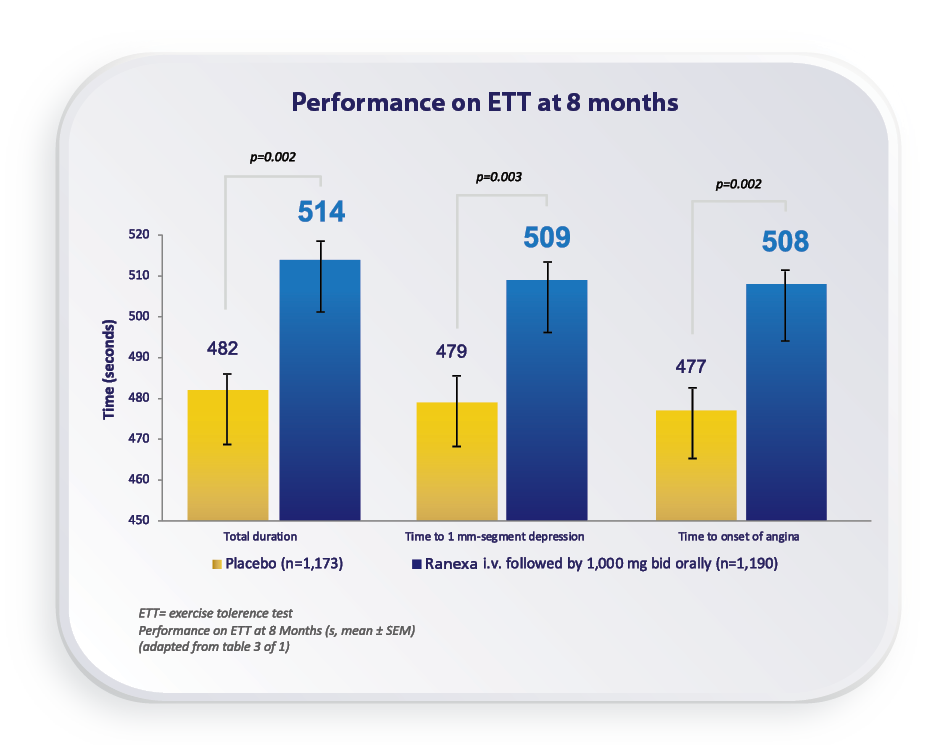
Ranexa significantly improved all measures of exercise performance among the patients with ACS and prior chronic angina.1
For more details
Symptomatic Patient on Beta Blockers - History
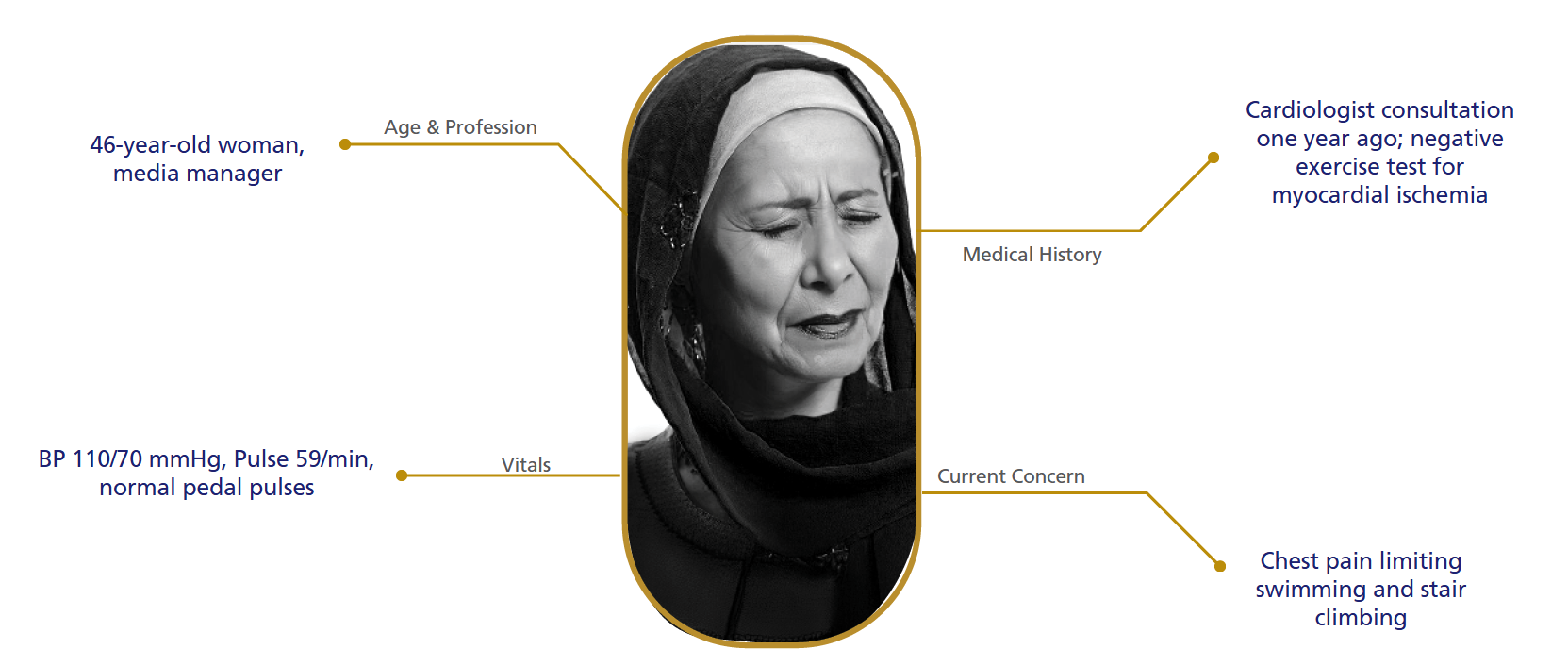
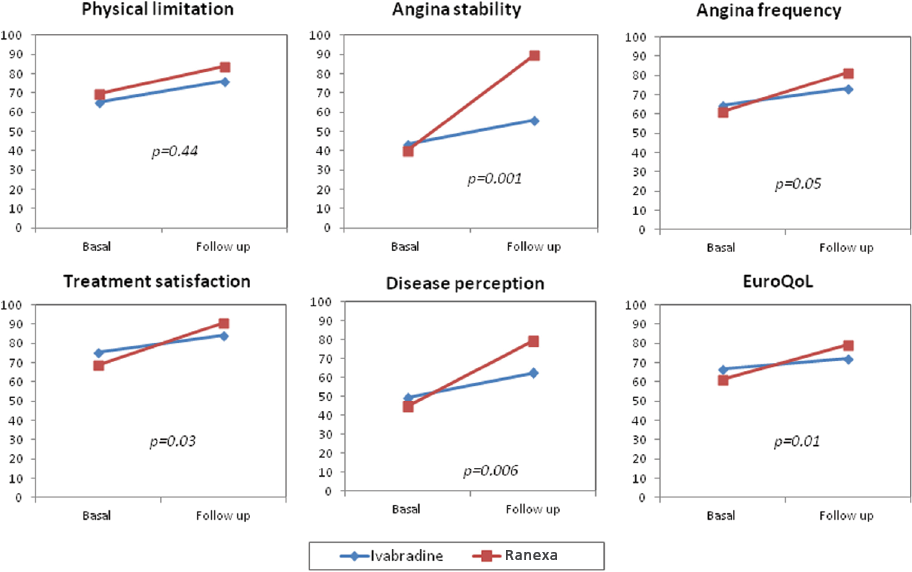
Ranexa Enhances Quality of Life and Symptom Control in Patients with Microvascular Angina.1
For more details
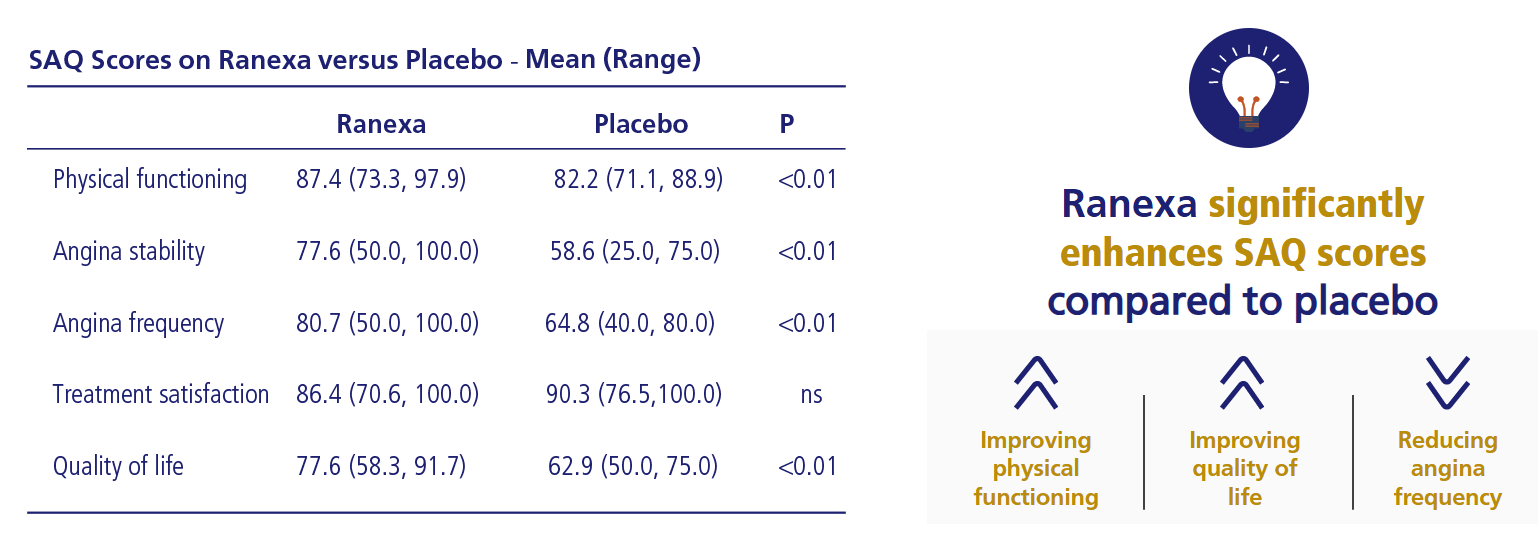
Ranexa Enhances Physical Functioning and Quality of Life1
Study details
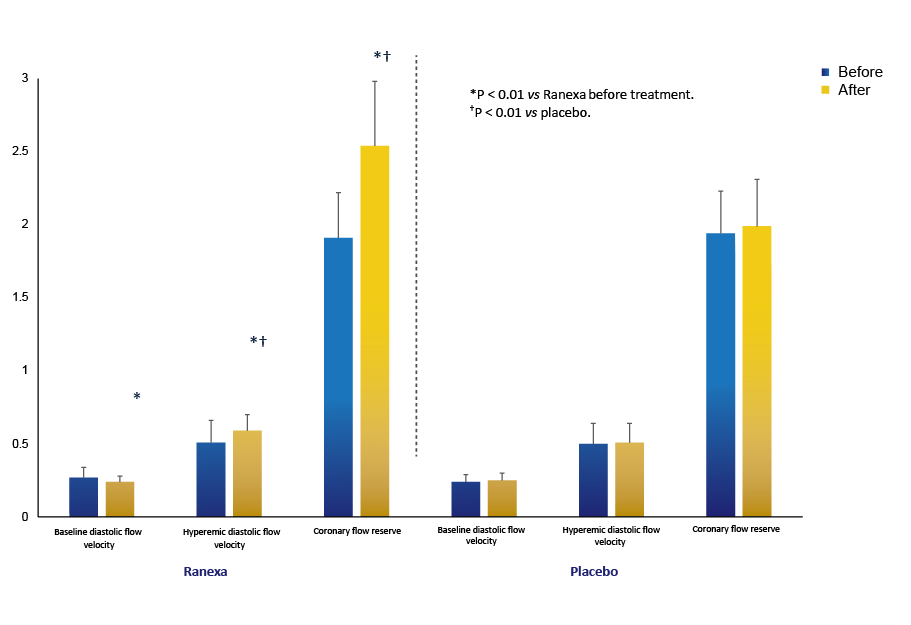
Ranexa Improves Coronary Flow Reserve
in Microvascular Angina1
For more details
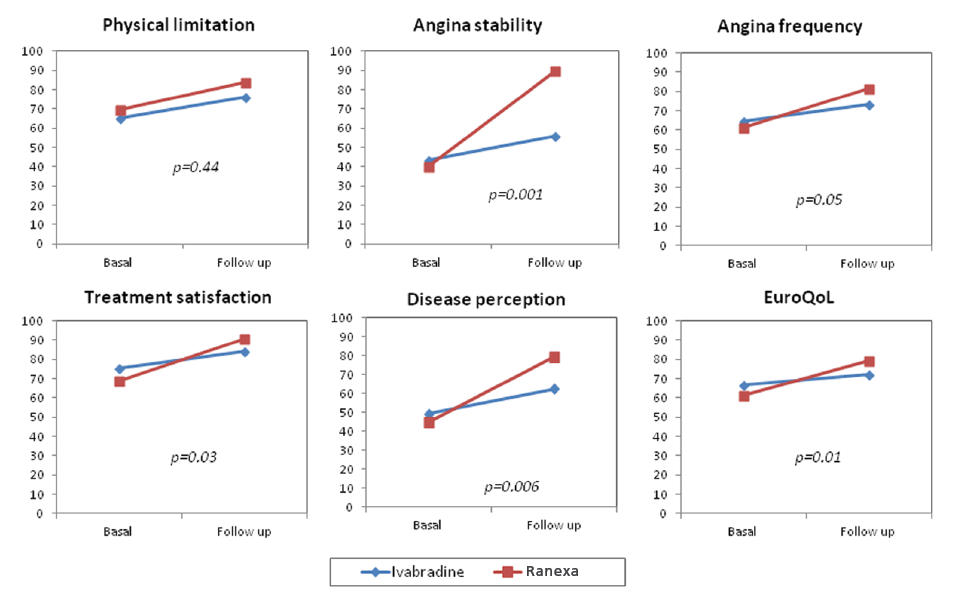
Ranexa’s Enhances Coronary Microvascular Function in Nonobstructive CAD1
Ranexa improves
3 of the 5 SAQ subscales:

Study details
Ranexa’s Enhances Coronary Microvascular Function in Nonobstructive CAD1
Ranexa improves
3 of the 5 SAQ subscales:
Study details
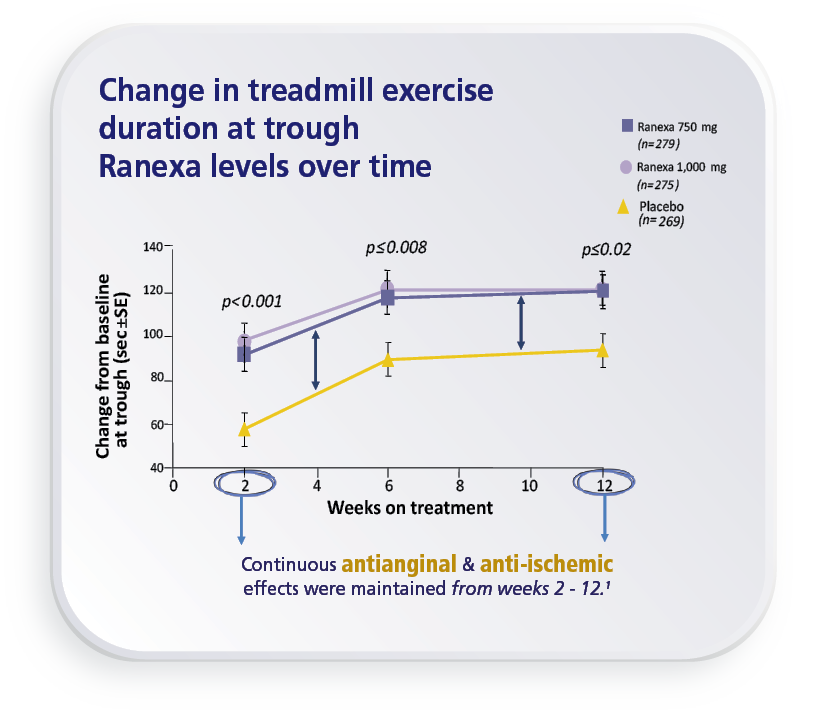
Efficacy of Ranexa


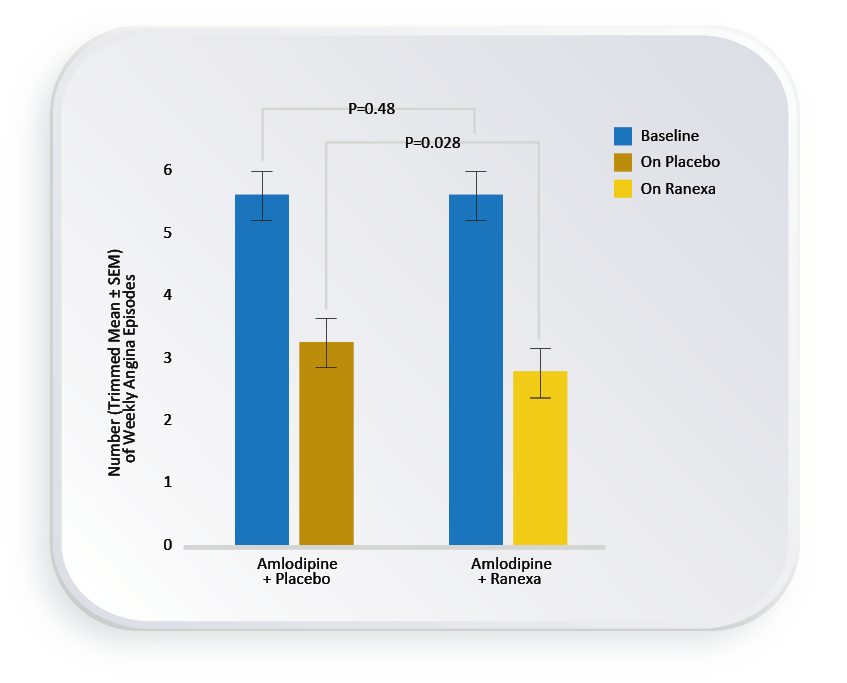
ERICA Study1

Ranexa provided significant additional antianginal benefit in patients who remained symptomatic despite maximum recommended therapy with a calcium channel blocker.1
For more details
TERISA study1

For more details
MERLIN-TIMI 36 Study: Ranexa’s Efficacy in Acute
Coronary Syndrome & Chronic Angina1,2
Ranexa significantly reduces cardiovascular endpoints and angina-related events compared to placebo.
For more details
CARISA Study1

Ranexa significantly increased
treadmill exercise duration by 46.3 Sec at peak drug levels.1 (p=0.006)
For more details
OSCAR Observational Study:
Real-World Evidence for Ranexa1
For more details

For more details
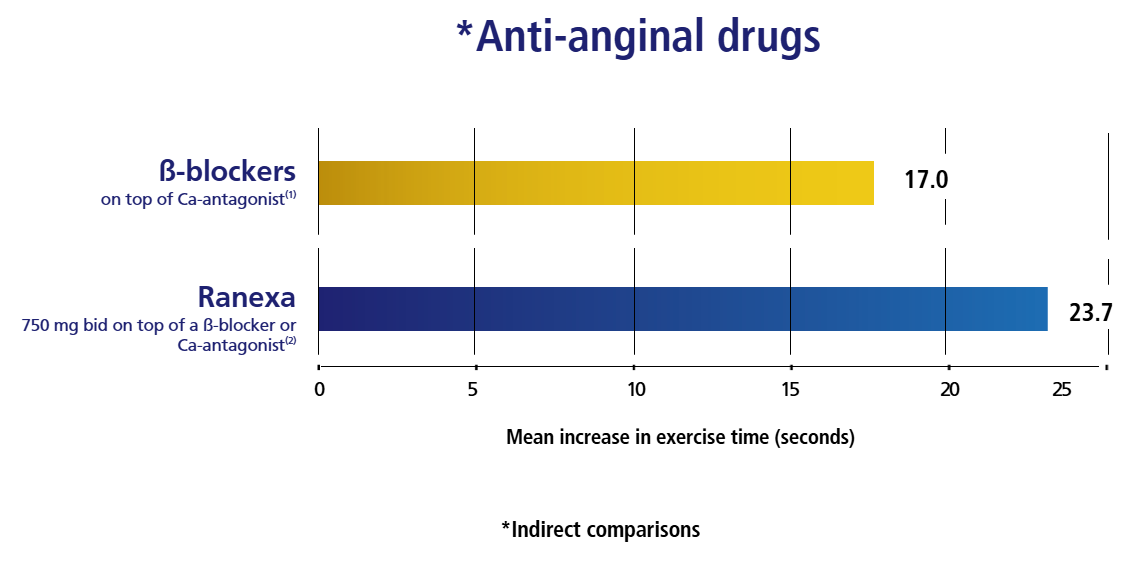
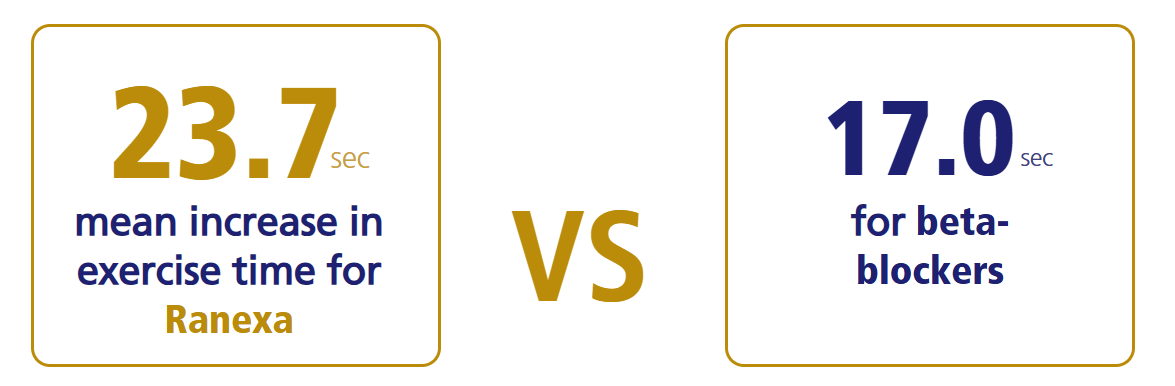
Ranexa VS Beta Blocker1,2
Ranexa improves patient endurance & symptom management with1,2
For more details
MERLIN-TIMI 36 Study1

Ranexa significantly improved all measures of exercise performance among the patients with ACS and prior chronic angina.1
For more details
Ranexa Enhances Quality of Life and Symptom Control in Patients with Microvascular Angina.1
For more details
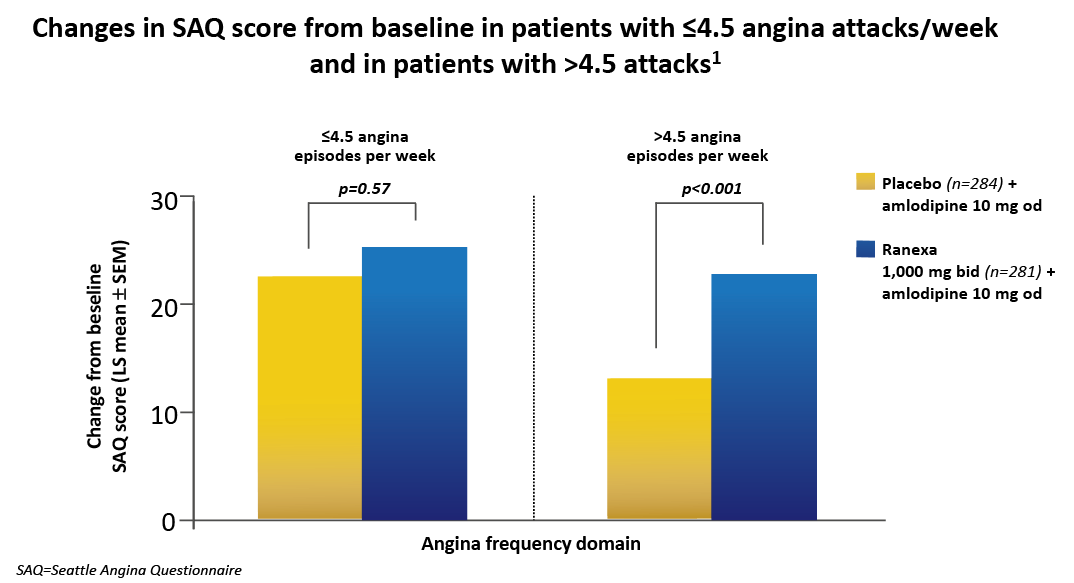
ERICA: Ranexa Significantly
Improves Quality of Life1
Ranexa significantly

for patients with >4.5 angina episodes per week, showing a substantial increase in SAQ scores compared to placebo.1
For more details
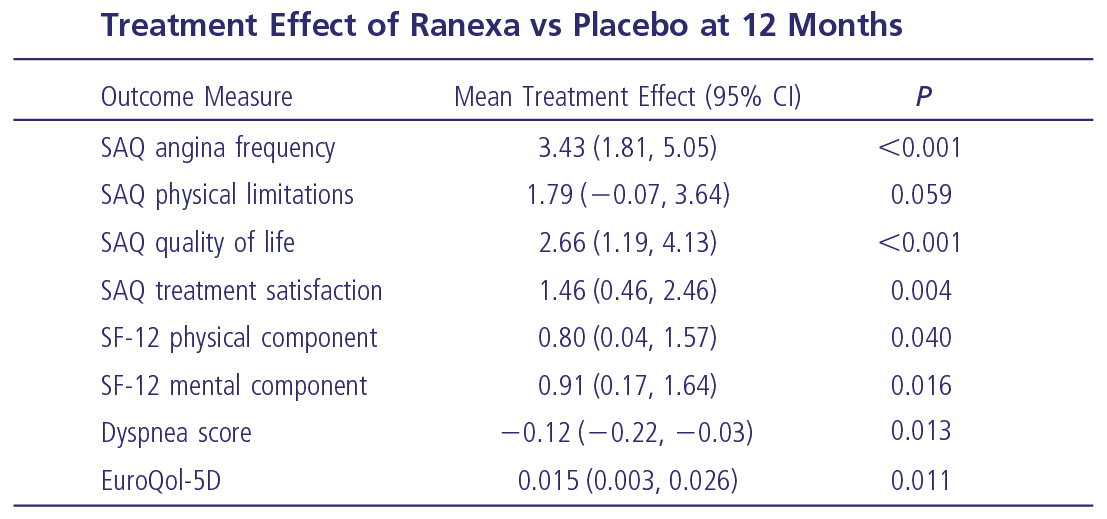
Ranexa Significantly Improves Quality of Life1,2
For more details
ARETHA Study: Ranexa Transforming Quality of Life in Stable Angina Patients1
For more details
RANGER Study: The clinical efficacy of Ranexa has been proven in several large randomised, controlled clinical trials that overall enrolled more than 8,000 patients with coronary heart disease1
RANGER Study: Real-World Data for Ranexa in Stable Angina1
For more details

For more details
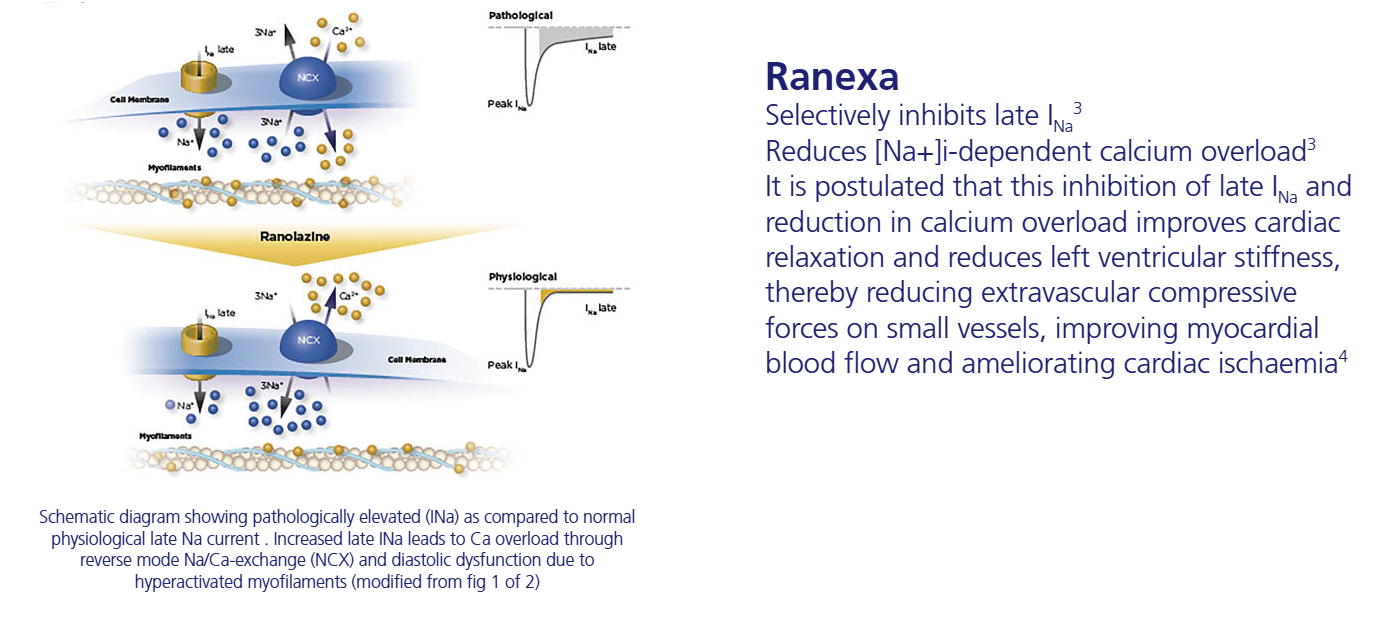
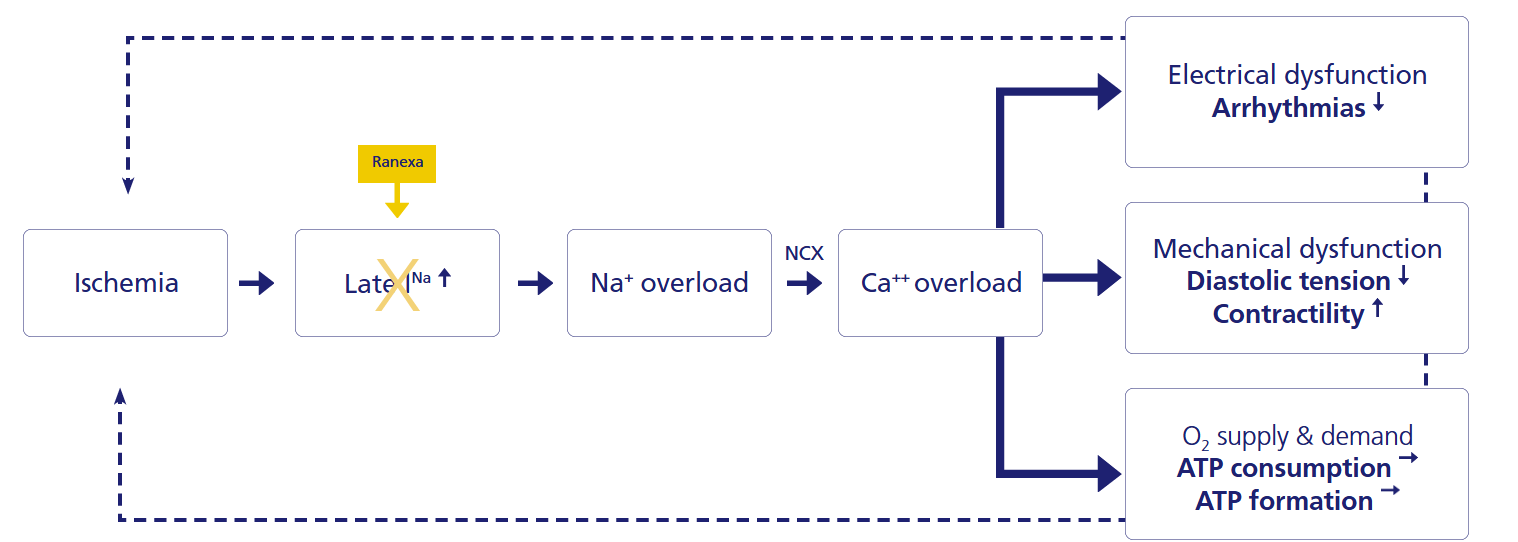
Ranexa Mechanism of Action1
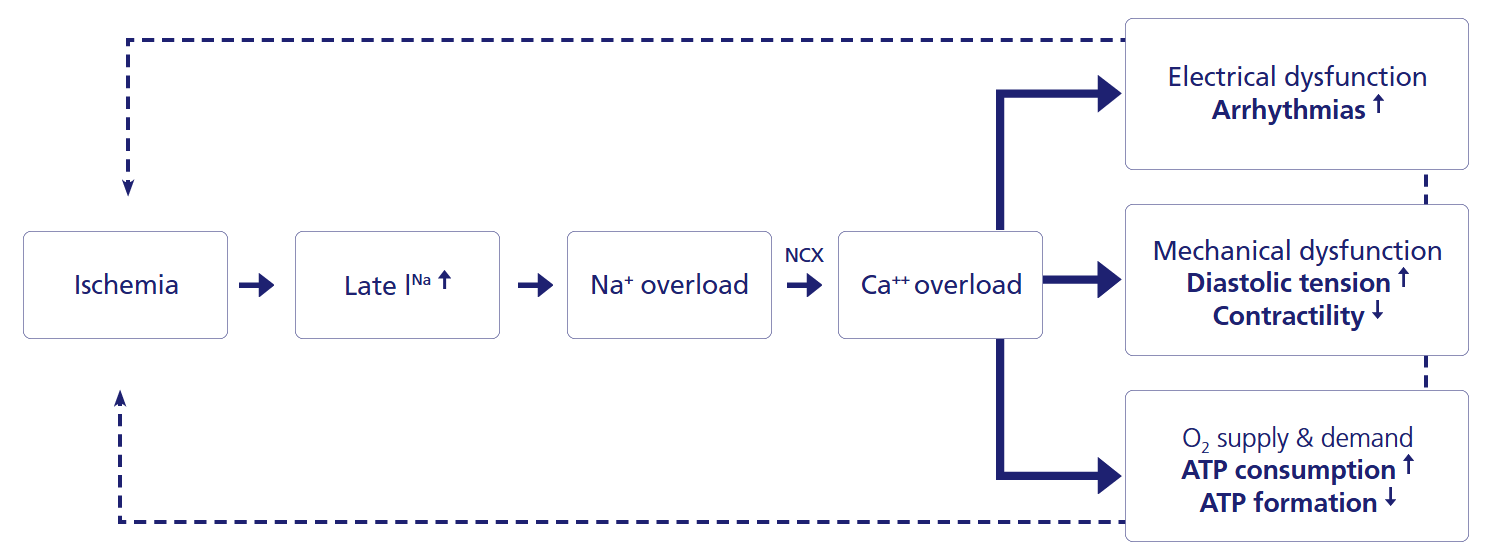
For more details
Ranexa Mechanism of Action1
For more details
ESC & ACC/AHA Guidelines Recommendations for Ranexa
For more details

For more details

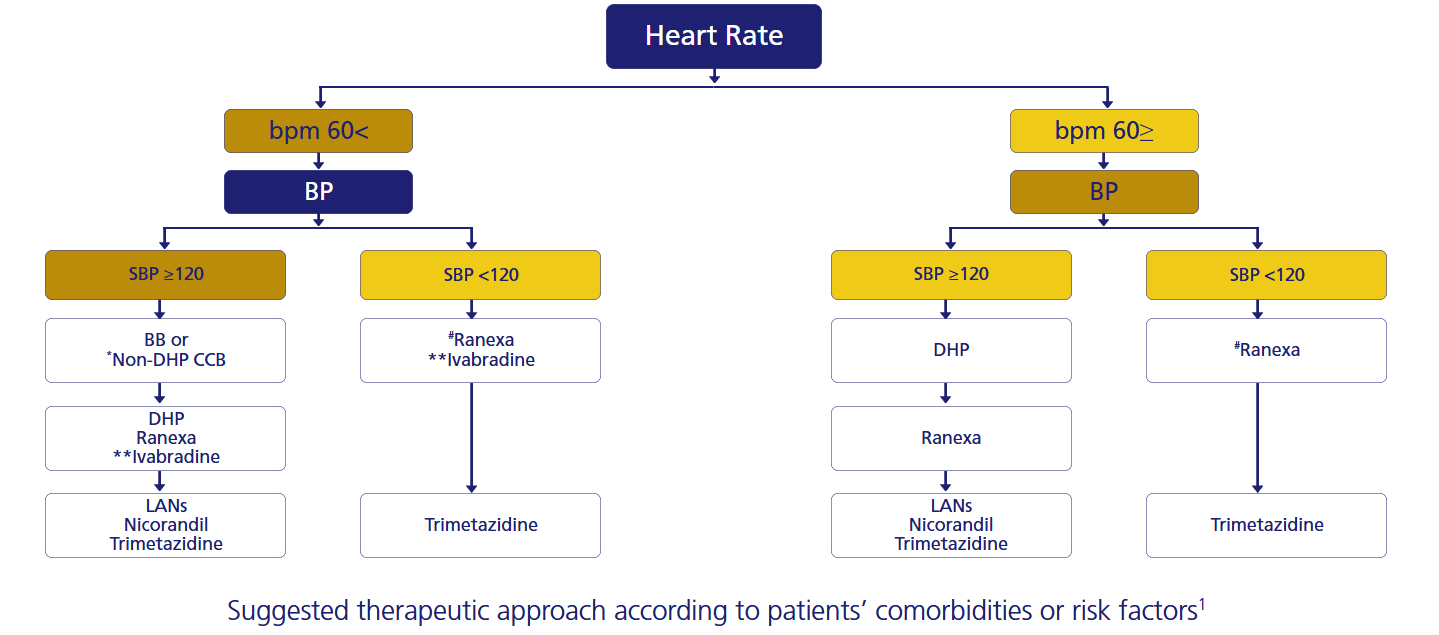
Tailored Therapeutic Approaches Suggested by Experts1,2
For more details
Choosing Among Antianginals
|
Blood pressure |
Heart rate |
|
|
Long-acting nitrate1 |
|
–— |
|
Ivabradine2 |
–— |
|
|
Nicorandil3 |
|
–— |
|
Diltiazem4 |
|
|
|
Amlodipine5 |
|
–— |
|
Atenolol6 |
|
|
|
Trimetazidine7 |
–— |
–— |







Ranexa effects do NOT depend upon changes in heart rate, blood pressure, or vasodilation.8

Long Acting Nitrates
|
Improvement9 |
ENDOTHELIAL FUNCTION |
Possible worsening10 |
|
No8 |
TOLERANCE |
Yes10 |
|
No8 |
REBOUND EFFECT |
Yes11 |
|
No substantial effect12 |
BLOOD PRESSURE |
Decrease1 |
|
No substantial effect12 |
HEART RATE |
Possible reflex tachycardia1 |
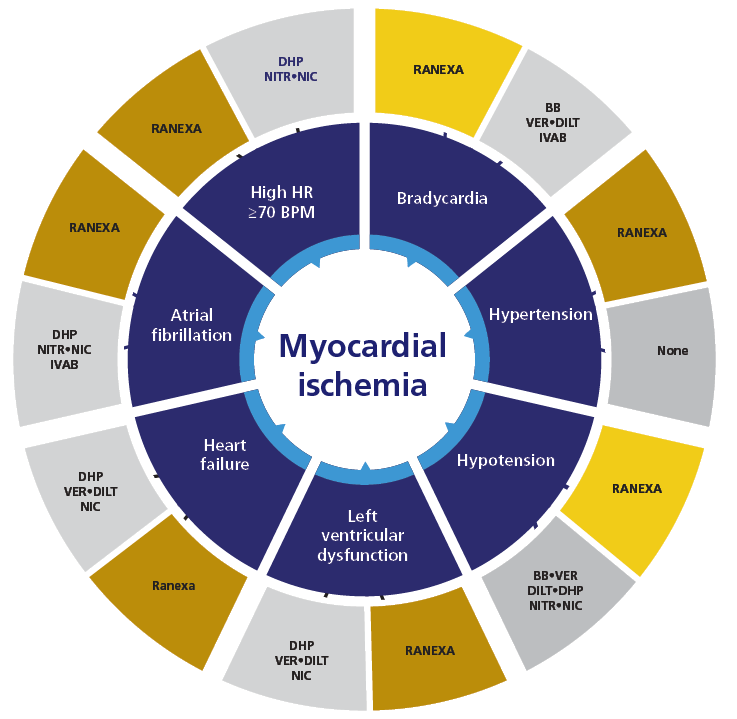
Therapeutic Approach Based on Comorbidities1
Safety1
Undesirable effects in patients receiving Ranexa® are generally mild to moderate in severity and often develop within the first 2 weeks of treatment. The adverse events reported as common (≥1/100 to <1/10) and considered to be at least possibly related to treatment were: dizziness, headache, constipation, vomiting, nausea and asthenia.1
There is a theoretical risk that concomitant treatment of Ranexa with other drugs known to prolong the QTc interval may give rise to a pharmacodynamic interaction and increase the possible risk of ventricular arrhythmias.
Examples of such drugs include certain antihistamines (e.g. terfenadine, astemizole, mizolastine), certain antiarrhythmics (e.g. quinidine, disopyramide, procainamide), erythromycin, and tricyclic antidepressants (e.g. imipramine, doxepin, amitriptyline).
Main contraindications:
- Severe renal impairment (creatinine clearance < 30 ml/min)
- Moderate or severe hepatic impairment
- Concomitant potent CYP3A4 inhibitors (e.g. itraconazole, ketoconazole, voriconazole, posaconazole, HIV protease inhibitors, clarithromycin, telithromycin, nefazodone)
- Class Ia (e.g. quinidine) or Class III (e.g. dofetilide, sotalol) antiarrhythmics other than amiodarone
Careful dose titration is recommended in:
- Concomitant administration of moderate CYP3A4 inhibitors (e.g. diltiazem, fluconazole, erythromycin)
- Concomitant administration of P-gp inhibitors (e.g. verapamil, ciclosporin)
- Mild hepatic impairment
- Mild to moderate renal impairment (creatinine clearance 30–80 ml/min)
- Elderly
- Patients with low weight (≤ 60 kg)
- Patients with moderate to severe CHF (NYHA Class III–IV)
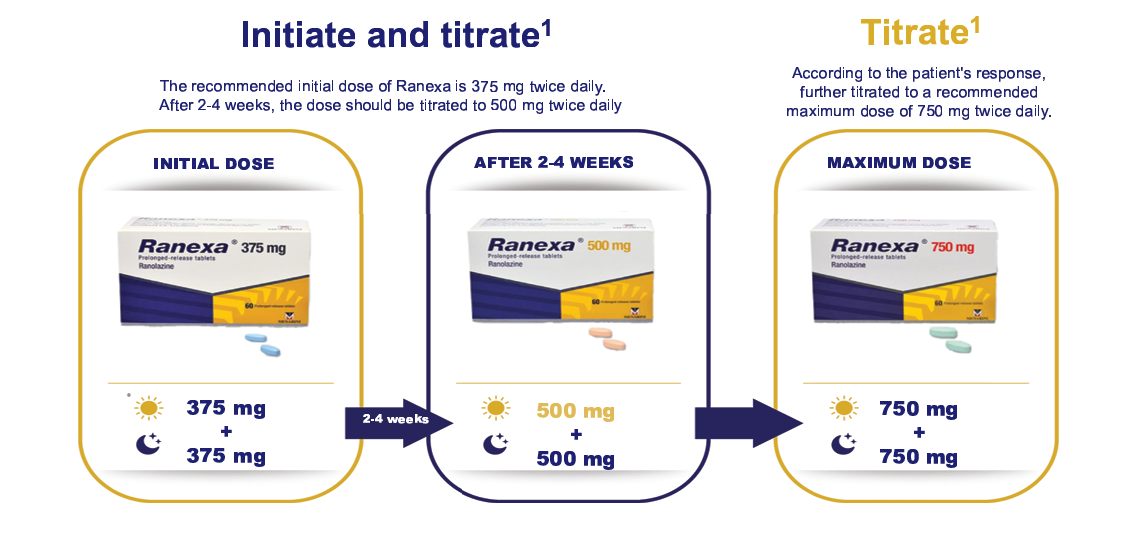
Posology and Method of Administration1
Ranexa is indicated in adults as add-on therapy for the symptomatic treatment of patients with stable angina pectoris who are inadequately controlled or intolerant to first-line antianginal therapies (such as beta-blockers and/or calcium antagonists)
For Ranexa SmPC

For Ranexa SmPC